Guideline 12.5 – Management after Return of Spontaneous Circulation (ROSC)
Summary
ANZCOR Guidelines 12.1 to 12.5 are provided to assist health professionals in the resuscitation of children. Differences from the adult and newborn guidelines reflect differences in the causes of cardiorespiratory arrest in, and anatomy and physiology of newborns, older infants, children and adults. These guidelines draw from the Paediatric Life Support 2025 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations,1 the development of which included representation from the Australian and New Zealand Committee on Resuscitation
(ANZCOR). The 2025 European Resuscitation Council Paediatric Life Support guidelines,2 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Care,3, 4 previous Paediatric Life Support International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations5-25statements and local practices have also been considered.
ANZCOR Guideline 12.5 focuses on the management of the infant or child after cardiorespiratory arrest in cases where return of spontaneous circulation has been achieved. It should be read in conjunction with the other paediatric guidelines (ANZCOR Guidelines 12.1, 12.2, 12.3 and 12.4).
To whom does this guideline apply?
This guideline applies to infants and children (refer to ANZCOR Guideline 12.1 for definitions) who have return of spontaneous circulation (ROSC) after cardiorespiratory arrest.
Who is the audience for this guideline?
This guideline is intended for health professionals who care for infants and children in healthcare environments where resuscitation equipment and medications are available.
It represents the next steps in the continuum of care from bystander basic life support (BLS) and/or health professional paediatric basic life support (PBLS) and paediatric advanced life support (PALS) through to recovery and steps to optimise long term outcome.
About this Guideline
|
Search date/s |
ILCOR literature search details and dates are available on the CoSTR page of the ILCOR website (https://costr.ilcor.org) and relevant CoSTR documents. |
|
Questions/PICOs: |
Are described in the CoSTR documents (https://costr.ilcor.org) |
|
Method: |
The guideline process includes involvement of stakeholders from member organisations of the Australian Resuscitation Council & New Zealand Resuscitation Council, and peer review by members of the Australian and New Zealand Committee on Resuscitation (ANZCOR). Details of the guideline development process can be found on the ANZCOR website at www.anzcor.org. The ANZCOR treatment recommendations provided (highlighted in grey boxes) bring together the available resuscitation evidence and clinical expertise. If an ANZCOR treatment recommendation is obtained from the ILCOR CoSTR, that statement will be referenced. Where the development of a recommendation has been based on “expert consensus opinion”, this will be labelled as either an ILCOR Good Practice Statement or an ANZCOR Good Practice Statement. Some paediatric doses are provided for reference but practitioners should comply with local drug dosing guidelines. |
|
Principal reviewers: |
Jason Acworth, Marissa Alexander, Christine Brabyn, Jane Cichero, Elliot Long, Andrea Christoff, Gabrielle Nuthall |
|
Approved: |
April 2026 |
Abbreviations
|
Abbreviation |
Meaning/Phrase |
|
ALS |
advanced life support |
|
ANZCOR |
Australian and New Zealand Committee on Resuscitation |
|
BLS |
basic life support |
|
BP |
blood pressure |
|
CoSTR |
Consensus on Science with Treatment Recommendations |
|
CPR |
cardiopulmonary resuscitation |
|
ECG |
electrocardiogram |
|
EEG |
electroencephalogram |
|
EIT |
Education, Implementation and Teams |
|
ETT |
endotracheal tube |
|
IHCA |
in-hospital cardiac arrest |
|
ILCOR |
International Liaison Committee on Resuscitation |
|
IO |
intraosseous |
|
IV |
intravenous |
|
OHCA |
out-of-hospital cardiac arrest |
|
PaCO2 |
partial pressure of arterial carbon dioxide |
|
PaO2 |
partial pressure of arterial oxygen |
|
PALS |
paediatric advanced life support |
|
PBLS |
paediatric basic life support |
|
PLS |
paediatric life support |
|
PCAS |
post cardiac arrest syndrome |
|
RCT |
randomised control trial |
|
ROSC |
return of spontaneous circulation |
|
SGA
SCA |
supraglottic airway
sudden cardiac arrest |
|
TTM |
targeted temperature management |
Summary of Changes
The main changes made in this latest update to the ANZCOR Guideline 12.5 include:
|
Section |
Updated Guidance |
Previous Guidance |
|
1.0 |
ANZCOR suggests that infants and children with ROSC who have been resuscitated after cardiorespiratory arrest should be admitted to a facility with the necessary resources for post cardiac arrest care. |
ANZCOR suggests that infants and children with ROSC who have been resuscitated after cardiorespiratory arrest should be admitted to a facility with the necessary resources for proper post-ROSC neuroprotective care, organ- and/or life supporting treatments, comprehensive neurological assessment and psychosocial support. |
|
2.0 |
ANZCOR recommends that for infants and children after ROSC, a systolic or mean arterial blood pressure >10th percentile for age should be targeted. |
ANZCOR recommends that for infants and children after ROSC, parenteral fluids and/or inotropes or vasopressors should be used to maintain a systolic blood pressure of at least greater than the fifth percentile for age. |
|
3.0 |
ANZCOR suggests that rescuers measure partial pressure of arterial carbon dioxide (PaCO2) after ROSC and target normocapnia. Consider adjustments to the target PaCO2 for specific patient populations where normocapnia may not be desirable (e.g. chronic lung disease, congenital heart disease, increased intracranial pressure). ANZCOR suggests that rescuers measure partial pressure of arterial oxygen (PaO2) after ROSC and target a value appropriate to the specific patient condition and suggest rescuers target normoxemia after ROSC. ANZCOR suggests that, to achieve normoxia, targeting an oxygen saturation of 94 to 99% may be a reasonable alternative to measuring PaO2.
|
ANZCOR suggests that rescuers measure PaCO2 after ROSC and target normocapnia. Consider adjustments to the target PaCO2 for specific patient populations where normocapnia may not be desirable (e.g. chronic lung disease with chronic hypercapnia, congenital heart disease with single-ventricle physiology, increased intracranial pressure with impending herniation). ANZCOR suggests that rescuers measure PaO2 after ROSC and target a value appropriate to the specific patient condition. In the absence of specific patient data, we suggest rescuers target normoxemia after ROSC. Given the availability of continuous pulse oximetry, targeting an oxygen saturation of 94% to 99% may be a reasonable alternative to measuring PaO2 and titrating oxygen when feasible to achieve normoxia. |
|
6.0 |
ANZCOR suggests continuous electroencephalogram (EEG) monitoring should be considered post-arrest within the first 24 hours and the treatment of seizures is suggested for children post–cardiac arrest. Routine use of prophylactic anti-seizure medication is not advised. |
Nil |
|
7.0 |
ANZCOR recommends that no single test be used in isolation to predict good neurological outcome in children after cardiac arrest. Clinicians should use multiple tests in combination for good neurological outcome prediction. ANZCOR recommends that no single test be used in isolation to predict poor neurological outcome in children after cardiac arrest. Clinicians should use multiple tests in combination for poor neurological outcome. |
ANZCOR suggests that practitioners use multimodal tools to predict neurologic outcomes for infants and children after cardiac arrest. |
|
9.0 |
ANZCOR suggests performing post-event debriefing after paediatric cardiac arrest in all settings. |
ANZCOR suggests data-driven, performance-focused debriefing of rescuers after IHCA or OHCA in children. |
Introduction
After the return of spontaneous circulation (ROSC), resuscitation does not stop. It is essential to continue maintenance of airway, breathing and circulation. ROSC is just the first step toward the goal of complete recovery from cardiac arrest.
Return of circulation following successful resuscitation results in the complex physiology of post cardiac arrest syndrome (PCAS). The key components of this are:
1. post cardiac arrest brain injury
2. post cardiac arrest myocardial dysfunction
3. systemic ischemia/reperfusion response
4. the persistent precipitating pathophysiology of the cardiac arrest.
To maximise survival to hospital discharge with good neurological outcome, these components must all be anticipated, recognised and treated.
Hypoxic brain injury, myocardial injury or subsequent organ failure are the predominant causes of morbidity and mortality after cardiac arrests. The goal of post-cardiac arrest care is to prevent ongoing secondary brain injury and optimise end-organ perfusion to allow time for recovery and ongoing neuroprognostication.
The possible reversible causes of cardiorespiratory arrest should be sought and treated. Reversible causes (the “4Hs and 4Ts”) include hypoxaemia, hypovolaemia, hypo/hyperthermia, hyper/hypokalaemia or other metabolic disorders, cardiac tamponade, tension pneumothorax, toxins, (poisons and drugs) and thrombosis (cardiac or pulmonary).
Occasionally, cardiac arrest occurs unexpectedly in an infant or child. In the case of sudden cardiac arrest (SCA), a standardised diagnostic protocol should be used to identify the cause of arrest event. If the SCA might have been due to an inherited condition, such as certain arrhythmias and cardiomyopathies, appropriate screening of family members should be considered.
It is important to use a systematic approach to post cardiac arrest management supporting end organ function and treating PCAS should commence immediately after ROSC. Use individualised goals and bundles of care and treat underlying disease. Patients should be transferred to centres where ongoing paediatric intensive care therapies can be provided. Intensive care monitoring includes electrocardiogram (ECG), pulse oximetry, capnography, temperature and blood pressure. Routine monitoring should also include invasive arterial blood pressure monitoring and central venous access in all comatose children.
ANZCOR suggests that infants and children with ROSC who have been resuscitated after cardiorespiratory arrest should be admitted to a facility with the necessary resources for post-cardiac arrest care [ANZCOR Good Practice Statement].
Post ROSC Haemodynamic Support
It is important to ensure an adequate systemic arterial blood pressure as soon as practicable after ROSC. The known pathophysiology of post-cardiac arrest syndrome provides a rationale for titrating haemodynamic support to optimise organ perfusion.26 Blood pressure should ideally be monitored using continuous arterial line pressure monitoring, so hypotension can be rapidly identified and treated. Any episode of hypotension may be associated with worse neurologic outcomes.26-29
The topic of post-ROSC blood pressure targets was most recently reviewed as part of the CoSTR 2025 process.1Optimal blood pressure (BP) targets in infants and children following return of circulation after cardiac arrest are not well defined. New evidence emerged after the systematic review,1 prompting an updated systematic review.30 Seven non-randomised observational cohort studies were included, 5 of which were secondary analyses.
ANZCOR recommends that for infants and children after ROSC, a systolic or mean arterial blood pressure >10th percentile for age should be targeted [CoSTR 2025, weak recommendation, very low certainty evidence].
BP percentile ranges for age are available for reference.31, 32
Post ROSC Oxygenation and Ventilation
Optimal oxygenation and ventilation of children after ROSC may be altered by the pathology that caused the cardiac arrest and post-cardiac arrest ischemic injury and reperfusion. For management of oxygenation and ventilation, PaO2, PaCO2 and saturations should be monitored. Target normoxia and/or saturations of 94 to 99% (or child’s normal oxygen saturations), and avoid hypocapnia (or aim for a PaCO2 that is appropriate for the child’s underlying condition).33-36
As a part of the ILCOR 2020 CoSTR process, a systematic review37 of oxygen and carbon dioxide targets in adults and children with ROSC after cardiac arrest was conducted with involvement of clinical content experts from both the adult life support (ALS) and paediatric life support (PLS) Task Forces. Evidence from adult and paediatric literature was sought and considered by the ALS and PLS Task Forces, respectively.
No paediatric randomised control trials (RCTs) were identified examining ventilation and oxygenation post ROSC in children. Observational studies34, 36 showed an increase in hospital mortality associated with both hypocapnia and hypercapnia after ROSC compared with normocapnia. No benefit was found for hyperoxemia compared with normoxemia.34, 38, 39 One large registry-based study40 found that hyperoxemia was associated with higher mortality when compared with normoxemia.
An ILCOR systematic review is being undertaken to review new evidence for post ROSC ventilation and oxygenation and association with critical outcomes of survival to hospital discharge and survival with favourable neurologic outcome in children.
ANZCOR suggests that rescuers measure PaCO2 after ROSC and target normocapnia [CoSTR 2020 weak recommendation, very low-certainty evidence]. Consider adjustments to the target PaCO2 for specific patient populations where normocapnia may not be desirable (e.g. chronic lung disease, congenital heart disease, increased intracranial pressure).
ANZCOR suggests that rescuers measure PaO2 after ROSC and target normoxemia. A value appropriate to the specific patient condition should be chosen [CoSTR 2020, weak recommendation, very low-quality evidence].
ANZCOR suggests that, to achieve normoxia, targeting an oxygen saturation of 94-99% may be a reasonable alternative to measuring PaO2 [Good Practice Statement].
Temperature Management
Elevated core body temperature is common after cardiac arrest. Persistent hyperthermia is associated with unfavourable neurological outcomes in children.26 Timely continuous core temperature monitoring and active methods to achieve targeted temperature management (TTM) should be used for patients who are comatose after ROSC.
A systematic review addressing TTM was published in 2019,41 and an ILCOR Paediatric CoSTR was published as part of the 2019 CoSTR summary.17 In 2021, an evidence update was performed by the ILCOR PLS Task Force but did not identify sufficient new data to warrant repeating a systematic review.
On the basis of 2 randomised trials and multiple retrospective observational cohort studies that provided comparative data on favourable neurological outcome, survival, and in-hospital adverse events, there was inconclusive evidence to support or refute the use of induced hypothermia (32 0C to 34 0C) compared with active control of temperature at normothermia (36 0C to 37.5 0C) for children who achieve ROSC but remain comatose after out-of-hospital cardiac arrest (OHCA) or in-hospital cardiac arrest (IHCA).
ANZCOR suggests that for infants and children who remain comatose following ROSC from OHCA or IHCA, active control of temperature be used to maintain a central temperature of ≤37.5 0C [CoSTR 2019, weak recommendation, moderate-certainty evidence].
Glucose Control
Both hypoglycaemia and hyperglycaemia have been associated with unfavourable outcomes in critically ill children.26 Randomised control trials performed in both critically ill adults and children using insulin infusions to maintain glucose control42 have shown mixed results with concerns about impact of hypoglycaemic events on long term patient outcomes.43 A recent paediatric randomised controlled trial of lower-target glucose versus higher-target glucose control was ceased early due to low likelihood of benefit and the possibility of harm.26
There is currently insufficient evidence to determine the optimal blood glucose level during PCAC that is associated with improved neurological outcomes for infants and children.
ANZCOR suggests that blood glucose levels should be monitored after cardiac arrest with the aim of maintaining normoglycaemia. If insulin is used to control hyperglycaemia, care should be taken to avoid hypoglycaemia [ANZCOR Good Practice Statement].
Post ROSC Seizure Management
Both non-convulsive and convulsive seizures are common in the post ROSC phase. If resources allow, continuous electroencephalography (EEG) monitoring is recommended as, without this, non-convulsive seizure and non-convulsive status cannot be detected. While there is insufficient evidence to demonstrate that treatment of seizures improves outcome, both convulsive and non-convulsive seizures are associated with worse outcomes, and it is reasonable to treat seizures in consultation with experts.44, 45
A systematic review examining seizure prevention and management after cardiac arrest was published as part of the 2024 CoSTR summary.46 No paediatric studies reported improvement in survival with favourable neurological outcome or survival with prophylactic anti-seizure medication or treatment of seizures.
ANZCOR suggests continuous EEG monitoring should be considered post-arrest within the first 24 hours and the treatment of seizures is suggested for children post–cardiac arrest [ANZCOR Good Practice Statement]. Routine use of prophylactic anti-seizure medication is not advised [ILCOR Good Practice Statement]
Prognosis and Prediction of Outcome
The ILCOR PLS Task Force performed systematic reviews examining post-ROSC predictive factors associated with good neurological outcome in 20238, 47 and poor neurological outcome in 2025.1 Tests that have been found to be useful, non-discriminating, and not useful are summarised in Figures 1 and 2.
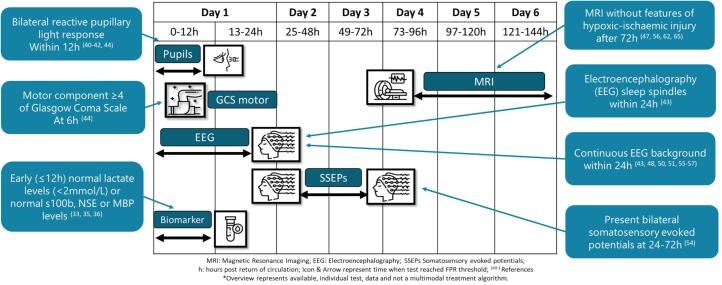
Figure 1: Overview of test and timing for prediction of good neurological outcome after paediatric cardiac arrest
[Reproduced from Scholefield et al https://doi.org/10.1016/j.resuscitation.2024.110483]
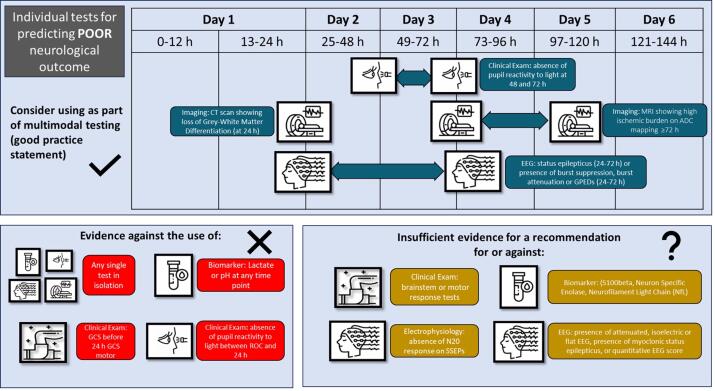
Figure 2: Overview of test and timing for prediction of poor neurological outcome after cardiac arrest
[Reproduced from Scholefield et al https://doi.org/10.1161/CIR.0000000000001362]
ANZCOR recommends that no single test be used in isolation to predict good neurological outcome in children after cardiac arrest. Clinicians should use multiple tests in combination for good neurological outcome prediction [ILCOR Good Practice Statement].
ANZCOR recommends that no single test be used in isolation to predict poor neurological outcome in children after cardiac arrest [CoSTR 2025, strong recommendation, very low–certainty evidence]. Clinicians should use multiple tests in combination for poor neurological outcome prediction [ILCOR Good Practice Statement].
Cessation of Cardiopulmonary Resuscitation
The decision to stop resuscitation efforts in paediatric patients after cardiac arrest is challenging. It should be based on a combination of factors including, but not limited to, the pre-arrest status, duration of arrest, response to resuscitation, remediable factors, opinions of experienced personnel and wishes of parents/carers.
Although there are no highly reliable means of determining outcome, in the absence of reversible causes, prolonged resuscitative efforts for children are unlikely to be successful.
It is important to note that the decision to stop resuscitation should not be made by a single individual but rather by a team of experienced healthcare professionals, including physicians, nurses, and other specialists, after following established guidelines and protocols. Additionally, the decision-making process may vary depending on local laws, cultural considerations, and institutional policies.
Post Cardiac Arrest debriefing
After resuscitation events staff may benefit from debriefing. This can be done either immediately after the event (hot debrief), or at a later time (cold debrief). It is increasingly recognised that there are a number of benefits to debriefing and that these include: acknowledgement of these events causing potential distress, clarifying medical facts and discovering both system successes and system improvements, which can all result in safer patient care.
The Education, Implementation and Teams (EIT) Taskforce performed a systematic review on debriefing of resuscitation performance as part of the ILCOR 2025 CoSTR process.48 The review was limited by high inconsistency (heterogeneity) across studies, reflecting variation in instructional design, provider type, and outcome measures. Performance of post-event debriefing was either associated with no effect or with improved outcome (favourable neurological outcome, survival to discharge, ROSC, chest compression depth, chest compression rate, chest compression fraction, adherence to guidelines). The review did not identify any undesirable effects (e.g. emotional trauma) related to debriefing after cardiac arrest in the reviewed studies and concluded that the reported positive effects outweigh any possible undesirable effects. The review also considered the high likelihood that this type of intervention is both acceptable to staff; with potential benefits such as improved teamwork, improved communication, or identification of latent safety threats.
ANZCOR suggests performing post-event debriefing after paediatric cardiac arrest in all settings [CoSTR 2025, weak recommendation, very low-certainty evidence].
References
1. Scholefield BR AJ, Ng K-C, Tiwari LK, Raymond TT, Christoff A, and Katzenschlager S E-KR, Bansal A, Topjian A, Kleinman M, Kurosawa H, Myburgh MC, del Castillo J, Rossano J, Djakow J, Guerguerian A-M, Nadkarni VM, Bittencourt Couto T, Schexnayder SM, Nuthall G, Tijssen JA, Ong GY-K, Gray JM, Lopez-Herce J, Ambunda ES, Nolan JP, Berg KM, Morrison LJ, Atkins DL, de Caen AR; on behalf of the Pediatric Life Support Task Force Collaborators. Pediatric life support: 2025 International Liaison Committee on Resuscitation Consensus on Science With Treatment Recommendations. Resuscitation. 2025;215.
2. Djakow J TN, Skellett S, Buysse CMP, Cardona F, de Lucas N, del Castillo J, Kiviranta P, Lauridsen KG, Markel F, Martinez-Mejias A, Roggen I, Biarent D, on behalf of the ERC Paediatric Life Support Writing Group Collaborators. European Resuscitation Council Guidelines 2025 Paediatric Life Support. Resuscitation. 2025;215.
3. Joyner BL DM, Bavare A, de Caen A, DiMaria K, Donofrio-Odmann J, Fosse G, Haskell S, Mahgoub M, Meckler G, Requist J, Schexnayder SM, Olech Smith M, Werho D, Raymond TT. Part 6: pediatric basic life support: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152:S424–S447.
4. Lasa JJ DG, Duff JP, Hayes J, Kamath-Rayne BD, Levy A, Mahgoub M, Morgan RW, McCormick T, Roberts JS, Ross CE, Schexnayder SM, Sweberg T, Valdes SO, Topjian AA. Part 8: pediatric advanced life support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152:S479–S537.
5. Greif R, Bray JE, Djarv T, Drennan IR, Liley HG, Ng KC, Cheng A, Douma MJ, Scholefield BR, Smyth M, Weiner G, Abelairas-Gomez C, Acworth J, Anderson N, Atkins DL, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2024;150:e580-e687.
6. Greif R, Bray JE, Djarv T, Drennan IR, Liley HG, Ng KC, Cheng A, Douma MJ, Scholefield BR, Smyth M, Weiner G, Abelairas-Gomez C, Acworth J, Anderson N, Atkins DL, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2024;205:110414.
7. Berg KM, Bray JE, Ng KC, Liley HG, Greif R, Carlson JN, Morley PT, Drennan IR, Smyth M, Scholefield BR, Weiner GM, Cheng A, Djarv T, Abelairas-Gomez C, Acworth J, et al. 2023 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2024;195:109992.
8. Berg KM, Bray JE, Ng KC, Liley HG, Greif R, Carlson JN, Morley PT, Drennan IR, Smyth M, Scholefield BR, Weiner GM, Cheng A, Djarv T, Abelairas-Gomez C, Acworth J, et al. 2023 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2023;148:e187-e280.
9. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, Scholefield BR, Smyth MA, Welsford M, Zideman DA, Acworth J, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Pediatrics. 2023;151.
10. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, Scholefield BR, Smyth MA, Welsford M, Zideman DA, Acworth J, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2022;181:208-288.
11. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, Scholefield BR, Smyth MA, Welsford M, Zideman DA, Acworth J, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2022;146:e483-e557.
12. Wyckoff MH, Singletary EM, Soar J, Olasveengen TM, Greif R, Liley HG, Zideman D, Bhanji F, Andersen LW, Avis SR, Aziz K, Bendall JC, Berry DC, Borra V, Bottiger BW, et al. 2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group. Circulation. 2022;145:e645-e721.
13. Wyckoff MH, Singletary EM, Soar J, Olasveengen TM, Greif R, Liley HG, Zideman D, Bhanji F, Andersen LW, Avis SR, Aziz K, Bendall JC, Berry DC, Borra V, Bottiger BW, et al. 2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group. Resuscitation. 2021;169:229-311.
14. Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Bittencourt Couto T, Guerguerian AM, Nadkarni VM, Ng KC, Nuthall GA, Ong GYK, Reis AG, Schexnayder SM, Scholefield BR, Tijssen JA, et al. Pediatric Life Support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Pediatrics. 2021;147.
15. Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Couto TB, Guerguerian AM, Nadkarni VM, Ng KC, Nuthall GA, Ong GYK, Reis AG, Schexnayder SM, Scholefield BR, Tijssen JA, et al. Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation. 2020;156:A120-A155.
16. Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Couto TB, Guerguerian AM, Nadkarni VM, Ng KC, Nuthall GA, Ong GYK, Reis AG, Schexnayder SM, Scholefield BR, Tijssen JA, et al. Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:S140-S184.
17. Soar J, Maconochie I, Wyckoff MH, Olasveengen TM, Singletary EM, Greif R, Aickin R, Bhanji F, Donnino MW, Mancini ME, Wyllie JP, Zideman D, Andersen LW, Atkins DL, Aziz K, et al. 2019 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2019;140:e826-e880.
18. Olasveengen TM, de Caen AR, Mancini ME, Maconochie IK, Aickin R, Atkins DL, Berg RA, Bingham RM, Brooks SC, Castren M, Chung SP, Considine J, Couto TB, Escalante R, Gazmuri RJ, et al. 2017 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Summary. Resuscitation. 2017;121:201-214.
19. Olasveengen TM, de Caen AR, Mancini ME, Maconochie IK, Aickin R, Atkins DL, Berg RA, Bingham RM, Brooks SC, Castren M, Chung SP, Considine J, Couto TB, Escalante R, Gazmuri RJ, et al. 2017 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Summary. Circulation. 2017;136:e424-e440.
20. de Caen AR, Maconochie IK, Aickin R, Atkins DL, Biarent D, Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM, Ng KC, Nuthall G, Reis AG, Shimizu N, Tibballs J, et al. Part 6: Pediatric Basic Life Support and Pediatric Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2015;132:S177-203.
21. Maconochie IK, de Caen AR, Aickin R, Atkins DL, Biarent D, Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM, Ng KC, Nuthall G, Reis AG, Shimizu N, Tibballs J, et al. Part 6: Pediatric basic life support and pediatric advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation. 2015;95:e147-68.
22. de Caen AR, Maconochie IK, Aickin R, Atkins DL, Biarent D, Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM, Ng KC, Nuthall G, Reis AG, Shimizu N, Tibballs J, et al. Part 6: Pediatric Basic Life Support and Pediatric Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations (Reprint). Pediatrics. 2015;136 Suppl 2:S88-119.
23. Kleinman ME, de Caen AR, Chameides L, Atkins DL, Berg RA, Berg MD, Bhanji F, Biarent D, Bingham R, Coovadia AH, Hazinski MF, Hickey RW, Nadkarni VM, Reis AG, Rodriguez-Nunez A, et al. Pediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1261-318.
24. de Caen AR, Kleinman ME, Chameides L, Atkins DL, Berg RA, Berg MD, Bhanji F, Biarent D, Bingham R, Coovadia AH, Hazinski MF, Hickey RW, Nadkarni VM, Reis AG, Rodriguez-Nunez A, et al. Part 10: Paediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation. 2010;81 Suppl 1:e213-59.
25. International Liaison Committee on R. 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Part 6: Paediatric basic and advanced life support. Resuscitation. 2005;67:271-91.
26. Topjian AA, de Caen A, Wainwright MS, Abella BS, Abend NS, Atkins DL, Bembea MM, Fink EL, Guerguerian AM, Haskell SE, Kilgannon JH, Lasa JJ and Hazinski MF. Pediatric Post-Cardiac Arrest Care: A Scientific Statement From the American Heart Association. Circulation. 2019;140:e194-e233.
27. Topjian AA, Telford R, Holubkov R, Nadkarni VM, Berg RA, Dean JM, Moler FW and Therapeutic Hypothermia After Pediatric Cardiac Arrest Trial I. Association of Early Postresuscitation Hypotension With Survival to Discharge After Targeted Temperature Management for Pediatric Out-of-Hospital Cardiac Arrest: Secondary Analysis of a Randomized Clinical Trial. JAMA Pediatr. 2018;172:143-153.
28. Topjian AA, French B, Sutton RM, Conlon T, Nadkarni VM, Moler FW, Dean JM and Berg RA. Early postresuscitation hypotension is associated with increased mortality following pediatric cardiac arrest. Crit Care Med. 2014;42:1518-23.
29. Perkins GD, Neumar R, Hsu CH, Hirsch KG, Aneman A, Becker LB, Couper K, Callaway CW, Hoedemaekers CWE, Lim SL, Meurer W, Olasveengen T, Sekhon MS, Skrifvars M, Soar J, et al. Improving Outcomes After Post-Cardiac Arrest Brain Injury: A Scientific Statement From the International Liaison Committee on Resuscitation. Circulation. 2024.
30. Nuthall G, Christoff A, Morrison LJ, Acworth J, Gray JM, Rossano J, Scholefield BR and International Liaison Committee on Resuscitation IPLSTF. Blood pressure targets after return of circulation following cardiac arrest in infants and children: a systematic review and meta-analysis. Resuscitation. 2025;216:110825.
31. Roberts JS, Yanay O and Barry D. Age-Based Percentiles of Measured Mean Arterial Pressure in Pediatric Patients in a Hospital Setting. Pediatr Crit Care Med. 2020;21:e759-e768.
32. Urbina E, Alpert B, Flynn J, Hayman L, Harshfield GA, Jacobson M, Mahoney L, McCrindle B, Mietus-Snyder M, Steinberger J, Daniels S, American Heart Association Atherosclerosis H and Obesity in Youth C. Ambulatory blood pressure monitoring in children and adolescents: recommendations for standard assessment: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the council on cardiovascular disease in the young and the council for high blood pressure research. Hypertension. 2008;52:433-51.
33. Frazier AH, Topjian AA, Reeder RW, Morgan RW, Fink EL, Franzon D, Graham K, Harding ML, Mourani PM, Nadkarni VM, Wolfe HA, Ahmed T, Bell MJ, Burns C, Carcillo JA, et al. Association of Pediatric Postcardiac Arrest Ventilation and Oxygenation with Survival Outcomes. Ann Am Thorac Soc. 2024;21:895-906.
34. Del Castillo J, Lopez-Herce J, Matamoros M, Canadas S, Rodriguez-Calvo A, Cechetti C, Rodriguez-Nunez A, Alvarez AC and Iberoamerican Pediatric Cardiac Arrest Study Network R. Hyperoxia, hypocapnia and hypercapnia as outcome factors after cardiac arrest in children. Resuscitation. 2012;83:1456-61.
35. Albrecht M, de Jonge RCJ, Del Castillo J, Christoff A, De Hoog M, Je S, Nadkarni VM, Niles DE, Tegg O, Wellnitz K, Buysse CMP and pedi RESQCI. Association of cumulative oxygen and carbon dioxide levels with neurologic outcome after pediatric cardiac arrest resuscitation: A multicenter cohort study. Resusc Plus. 2024;20:100804.
36. Lopez-Herce J, del Castillo J, Matamoros M, Canadas S, Rodriguez-Calvo A, Cecchetti C, Rodriguez-Nunez A, Carrillo A and Iberoamerican Pediatric Cardiac Arrest Study Network R. Post return of spontaneous circulation factors associated with mortality in pediatric in-hospital cardiac arrest: a prospective multicenter multinational observational study. Crit Care. 2014;18:607.
37. Holmberg MJ, Nicholson T, Nolan JP, Schexnayder S, Reynolds J, Nation K, Welsford M, Morley P, Soar J, Berg KM and Adult Pediatric Advanced Life Support Task Forces at the International Liaison Committee on R. Oxygenation and ventilation targets after cardiac arrest: A systematic review and meta-analysis. Resuscitation. 2020;152:107-115.
38. van Zellem L, de Jonge R, van Rosmalen J, Reiss I, Tibboel D and Buysse C. High cumulative oxygen levels are associated with improved survival of children treated with mild therapeutic hypothermia after cardiac arrest. Resuscitation. 2015;90:150-7.
39. Bennett KS, Clark AE, Meert KL, Topjian AA, Schleien CL, Shaffner DH, Dean JM, Moler FW and Pediatric Emergency Care Medicine Applied Research N. Early oxygenation and ventilation measurements after pediatric cardiac arrest: lack of association with outcome. Crit Care Med. 2013;41:1534-42.
40. Ferguson LP, Durward A and Tibby SM. Relationship between arterial partial oxygen pressure after resuscitation from cardiac arrest and mortality in children. Circulation. 2012;126:335-42.
41. Buick JE, Wallner C, Aickin R, Meaney PA, de Caen A, Maconochie I, Skrifvars MB, Welsford M and International Liaison Committee on Resuscitation Pediatric Life Support Task F. Paediatric targeted temperature management post cardiac arrest: A systematic review and meta-analysis. Resuscitation. 2019;139:65-75.
42. van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P and Bouillon R. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.
43. Agus MS, Wypij D, Hirshberg EL, Srinivasan V, Faustino EV, Luckett PM, Alexander JL, Asaro LA, Curley MA, Steil GM, Nadkarni VM, Investigators H-PS and the PN. Tight Glycemic Control in Critically Ill Children. N Engl J Med. 2017;376:729-741.
44. Herman ST, Abend NS, Bleck TP, Chapman KE, Drislane FW, Emerson RG, Gerard EE, Hahn CD, Husain AM, Kaplan PW, LaRoche SM, Nuwer MR, Quigg M, Riviello JJ, Schmitt SE, et al. Consensus statement on continuous EEG in critically ill adults and children, part II: personnel, technical specifications, and clinical practice. J Clin Neurophysiol. 2015;32:96-108.
45. Herman ST, Abend NS, Bleck TP, Chapman KE, Drislane FW, Emerson RG, Gerard EE, Hahn CD, Husain AM, Kaplan PW, LaRoche SM, Nuwer MR, Quigg M, Riviello JJ, Schmitt SE, et al. Consensus statement on continuous EEG in critically ill adults and children, part I: indications. J Clin Neurophysiol. 2015;32:87-95.
46. Greif R, Bray JE, Djärv T, Drennan IR, Liley HG, Ng K-C, Cheng A, Douma MJ, Scholefield BR, Smyth M, Weiner G, Abelairas-Gómez C, Acworth J, Anderson N, Atkins DL, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2024;0.
47. Scholefield BR, Tijssen J, Ganesan SL, Kool M, Couto TB, Topjian A, Atkins DL, Acworth J, McDevitt W, Laughlin S, Guerguerian AM, International Liaison Committee on R and Force IPLST. Prediction of good neurological outcome after return of circulation following paediatric cardiac arrest: A systematic review and meta-analysis. Resuscitation. 2025;207:110483.
48. Greif R CA, Abelairas-Gómez C, Allan KS, Breckwoldt J, Cortegiani A, Donoghue AJ, Eastwood KJ, Farquharson B, Hsieh M-J, Kidd T, Ko Y-C, Lauridsen KG, Lin Y, Lockey AS, Matsuyama T, Nabecker S, Nation KJ, Olaussen A, Schnaubelt S, Sawyer T, Yang C-W, Yeung J ; on behalf of the Education, Implementation, and Teams Task Force Collaborators. Education, implementation, and teams: 2025 International Liaison Committee on Resuscitation Consensus on Science With Treatment Recommendations. Resuscitation. 2025;215.
Referencing this guideline
When citing the ANZCOR Guidelines we recommend:
ANZCOR, 2026, Guideline 12.5 – Management after Return of Spontaneous Circulation (ROSC), accessed 10 August 2026, https://www.anzcor.org/home/paediatric-advanced-life-support/guideline-12-5-management-after-return-of-spontaneous-circulation-rosc
