Guideline 12.1 – Paediatric Basic Life Support (PBLS) for health professionals
Summary
Australian and New Zealand Committee on Resuscitation (ANZCOR) Guidelines 12.1 to 12.5 are provided to assist health professionals in the resuscitation of children. Differences from the adult and newborn guidelines reflect differences in the causes of cardiorespiratory arrest in, and anatomy and physiology of newborns, older infants, children and adults. These guidelines draw from the Paediatric Life Support 2025 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations,1 the development of which included representation from ANZCOR. The 2025 European Resuscitation Council Paediatric Life Support guidelines,2 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Care,3, 4 previous Paediatric Life Support International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations5-25statements and local practices have also been considered.
ANZCOR Guideline 12.1 focuses on provision of paediatric basic life support (PBLS) by health professionals responsible for the care of infants and children working in healthcare settings (pre-hospital or hospital). It recognises the importance of immediate provision of BLS in the collapsed child while waiting for resuscitative equipment and drugs to arrive, which then allow provision of paediatric advanced life support (PALS) as outlined in ANZCOR Guideline 12.2. This guideline should be read in conjunction with the other paediatric guidelines (ANZCOR Guidelines 12.2 to 12.5) and the general life support guidelines suitable for all age groups and environments (ANZCOR Guidelines 2 to 8).
To whom does this guideline apply?
This guideline applies to infants and children needing resuscitation excluding resuscitation of newborns (Refer to ANZCOR Guideline 12.1.2 for definitions).
Who is the audience for this guideline?
This guideline is intended for health professionals and those who respond to paediatric emergencies who have received training in PBLS practices. Lay rescuers and health professionals trained only in general basic life support (BLS) practices should refer to ANZCOR Guidelines 2 to 8 for general BLS procedures suitable for all age groups. Untrained rescuers should call emergency services and follow instructions from emergency dispatchers.
About this Guideline
|
Search date/s |
ILCOR literature search details and dates are available on the CoSTR page of the ILCOR website (https://costr.ilcor.org) and relevant CoSTR documents. |
|
Questions/PICOs: |
Are described in the CoSTR documents (https://costr.ilcor.org) |
|
Method: |
The guideline process includes involvement of stakeholders from member organisations of the Australian Resuscitation Council & New Zealand Resuscitation Council, and peer review by members of the Australian and New Zealand Committee on Resuscitation (ANZCOR). Details of the guideline development process can be found on the ANZCOR website at www.anzcor.org. The ANZCOR treatment recommendations provided (highlighted in grey boxes) bring together the available resuscitation evidence and clinical expertise. If an ANZCOR treatment recommendation is obtained from the ILCOR CoSTR, that statement will be referenced. Where the development of a recommendation has been based on “expert consensus opinion”, this will be labelled as either an ILCOR Good Practice Statement or an ANZCOR Good Practice Statement. Some paediatric doses are provided for reference but practitioners should comply with local drug dosing guidelines. |
|
Principal reviewers: |
Jason Acworth, Marissa Alexander, Christine Brabyn, Jane Cichero, Elliot Long, Andrea Christoff, Gabrielle Nuthall |
|
Approved: |
April 2026 |
Abbreviations
|
Abbreviation |
Meaning/Phrase |
|
AED |
automated external defibrillator |
|
ALS |
advanced life support |
|
ANZCOR |
Australian and New Zealand Committee on Resuscitation |
|
BLS |
basic life support |
|
BMV |
bag-mask ventilation |
|
CoSTR |
Consensus on Science with Treatment Recommendations |
|
CPR |
cardiopulmonary resuscitation |
|
FBAO |
foreign body airway obstruction |
|
IHCA |
in-hospital cardiac arrest |
|
ILCOR |
International Liaison Committee on Resuscitation |
|
OHCA |
out-of-hospital cardiac arrest |
|
PALS |
paediatric advanced life support |
|
PBLS |
paediatric basic life support |
|
PEA |
pulseless electrical activity |
|
PLS |
paediatric life support |
|
PPE |
personal protective equipment |
|
RCT |
randomised control trial |
|
ROSC |
return of spontaneous circulation |
Summary of Changes
The main changes made in this latest update to the ANZCOR Guideline 12.1 include:
|
Section |
Updated Guidance |
Previous Guidance |
|
8.0 |
Addition of statement: ANZCOR suggest that external cardiac compression should be started while rescuers wait for a bag-mask ventilation (BMV) device to arrive. If a BMV device is immediately available, 2 initial ventilations should be provided before commencement of external cardiac compression |
Always suggested 2 rescue breaths. |
|
9.0 |
Palpation of a pulse (or its absence) is not reliable as the sole determinant of cardiac arrest and need for chest compressions. ANZCOR suggest that, in infants and children who are unresponsive and breathing is absent (or agonal), healthcare providers should begin cardiopulmonary resuscitation (CPR). |
ANZCOR suggest that in infants and children who are unresponsive and not breathing normally, healthcare providers should begin CPR unless they can definitely palpate a pulse within 10 seconds. |
|
9.2 |
ANZCOR suggest that chest compression for an infant be performed with the two-thumb encircling technique as it results in consistently greater chest compression depth and less fatigue. Chest compression for an infant using the heel of one hand may be considered if the rescuer is unable to achieve optimal compression depth using the two-thumb encircling technique. |
Chest compression for an infant can be performed with two-thumb technique or two finger technique. The two-thumb technique is the strongly preferred technique for healthcare rescuers. |
|
10.0 |
CPR providers using manual defibrillation in infants and children, should place pads in an anterior-posterior position. |
Nil |
|
13.0 |
Addition of section on management of Foreign Body Airway Obstruction (FBAO) in children.
|
Refer to ANZCOR Guideline 4 |
Introduction
This guideline is provided by ANZCOR to assist health professionals who have been trained in paediatric basic life support (PBLS) and who are acting as first responders to significant clinical deterioration or cardiorespiratory arrest in infants and children in healthcare settings (and other environments). The guideline describes the initial vital steps to be performed by rescuers while they wait for other advanced practitioners, advanced equipment, and resuscitative drugs to become available.
The epidemiology, pathophysiology, and common aetiologies of paediatric cardiorespiratory arrest are quite different from those in adult or newborn arrest.26 Cardiorespiratory arrest in infants and children is not usually the result of a primary cardiac cause, but instead is the final result of progressive respiratory failure or shock. In the paediatric population, cardiorespiratory arrest is usually preceded by a period of deterioration, which may proceed to cardiorespiratory failure, bradycardia, and eventually, cardiorespiratory arrest. Even in children with congenital cardiac disease, where cardiorespiratory arrest may have a primary cardiac cause, the aetiology is often distinct from adults. That being said, early recognition and appropriate early management of children with a cardiac arrhythmia as a cause of their cardiac arrest is vital to provide the best chance of neurologically intact survival.
To reflect these differences, BLS guidelines have been tailored for the paediatric, newborn and adult populations. This must be balanced against the educational advantages of training using a general BLS algorithm.
ANZCOR suggest that [all ANZCOR Good Practice Statements]:
· Health professionals working in settings where they are responsible for the care of infants and children should be trained in paediatric basic life support (PBLS).
· Lay persons and other health professionals should be trained in general BLS.
Guideline 12.1 is focused on PBLS in healthcare settings, i.e. resuscitation without the aid of equipment and drugs to restore and maintain airway, breathing and circulation in infants and children.
Once equipment, medications (and often more experienced clinicians) arrive to help, paediatric advanced life support (PALS) should be seen as the next stage in the continuum from PBLS. Further details of PALS for infants and children can be found in ANZCOR Guideline 12.2.
Guideline 12.1 applies to children and infants. It does not refer in detail to the resuscitation of the newborn which can be found in ANZCOR Guidelines 13.1 to 13.10.
For health professionals caring for both adults and children, this guideline should act as an adjunct to the BLS guidelines for all age groups published by ANZCOR in Guidelines 2 to 8.
Terminology
Definitions of ‘newborn’, ‘infant’ and ‘child’ are based on combinations of physiology, age and physical size, which influence the efficacy and practicality of performing resuscitative techniques.
For the purposes of paediatric life support guidelines, paediatric patients include infants (0 to 12 months of age, i.e. up to their first birthday) and children (>12 months to <18 years), excluding newborns. The term ‘newborn’ refers to an infant in the first minutes to hours following birth.
From a practical perspective, if the rescuer believes that the patient is a child, then they should follow paediatric guidelines, and adult guidelines should be used for anyone who appears to be an adult. If the patient turns out to be a young adult, it is unlikely that any harm will have been done as the paediatric pattern of cardiorespiratory arrest has been demonstrated to continue into early adulthood.20
The exact age at which paediatric techniques, particularly the compression-ventilation ratio, should replace those used for newborns is not certain, especially for small premature infants. Infants whose cardiorespiratory physiology is in transition from an intra-uterine environment at birth to several hours after birth (i.e. newborns) should preferably be managed as per neonatal guidelines (Guidelines Section 13). Infants aged more than a few hours beyond birth should be managed according to paediatric guidelines (with a compression-ventilation ratio of 15:2) in the pre-hospital, emergency department, paediatric inpatient and paediatric intensive care unit environments.25
Sequence of actions in paediatric BLS by rescuers trained in paediatric BLS
The following sequence of actions (DRS ABCD) should be followed by health professionals acting in the role of first responder to a paediatric emergency:
- DANGERS? Check for danger (assess and manage risks to the rescuer and others)
- RESPONSIVE? Check for response (if unresponsive)
- SEND for HELP Call emergency services
- AIRWAY Open the airway
- BREATHING Check breathing
- CPR Start CPR (15 chest compressions followed by 2 ventilations)
- DEFIBRILLATION Attach manual defibrillator or an Automated External Defibrillator (AED) as soon as available and follow the prompts.
Dangers: ensure safety of the rescuer and the child
The personal safety of all individuals involved in resuscitation (patient and rescuers) is paramount. While there are very few reports of harm to rescuers during resuscitation, the following principles should apply:
- Always check that the environment and patient surroundings are safe before proceeding (to prevent harm to the rescuer).
- Personal protective equipment (PPE) should be used according to the perceived risk in the local setting.
Responsiveness: Assessment of response
The collapsed child's response to verbal and tactile stimuli should be assessed while also ensuring that this does not cause or aggravate any injury. This may include squeezing the shoulders firmly and asking loudly “Are you okay?”
If the child responds (e.g. by crying or moving), they should be left in a safe position and checked regularly while waiting for further help to arrive.
If the child is unresponsive, the rescuer should move immediately onto the next step in the sequence and call for help.
Sending for help
A single rescuer encountering an unwitnessed collapse of an infant or child should shout for help (and/or enact the local emergency response) then start CPR immediately.24 If help has not arrived within 1 minute, the rescuer should go to get help. To minimise interruptions to CPR, and if it safe to do so, it may be possible for the rescuer to carry the infant / small child with them while summoning help.
When more than one rescuer is available, one rescuer should start resuscitation while the other summons assistance.
ANZCOR suggest that a single first responder witnessing a sudden collapse (potential primary cardiac arrest) should prioritise obtaining help and then start CPR [ANZCOR Good Practice Statement].
Airway: Opening the airway
Airway opening manoeuvres, including backward head tilt with chin lift (Figures 1 & 2) or jaw thrust (Figures 3 & 4) may be used to optimise the position of the infant’s or child’s airway. Hyperextension of the neck should be avoided as it may cause airway obstruction, especially in small infants.
ANZCOR suggest that if a neck injury is suspected, only jaw thrust should be used to avoid worsening the injury [ANZCOR Good Practice Statement].

Figure 1: Head tilt with chin lift in an infant
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]

Figure 2: Head tilt with chin lift in a child
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]

Figure 3: Jaw thrust in an infant
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]

Figure 4: Jaw thrust in a child
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
The patency of the airway should be assessed by observation of movement of the chest and abdomen during breathing (LOOK), listening for breath sounds from the mouth or nose (LISTEN), and feeling for air movement on the rescuer’s cheek (FEEL) (Figure 5). An indrawing of the chest wall and/or distension of the abdomen with each inspiratory effort without expiration of air implies an obstructed airway.

Figure 5: Look, listen and feel assessment
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
Breathing: Assessing for normal breathing
Agonal respiration (gasping laboured breathing) describes an abnormal pattern of breathing (brainstem reflex) associated with cardiac arrest that should not be confused with normal breathing.
If breathing is absent (or agonal) despite airway repositioning, CPR should be commenced.
Despite the move towards chest compression only CPR to improve bystander CPR rates in untrained rescuers, most paediatric cardiac arrests are asphyxial in origin. In children, both ventilation and chest compressions are key components of CPR. ANZCOR places a higher value on the importance of ventilations as part of paediatric CPR over a strategy that deemphasises ventilation to simplify CPR instructions and skills.
ANZCOR suggest that PBLS trained rescuers provide ventilations and chest compressions for paediatric in-hospital cardiac arrest (IHCA) and out-of-hospital cardiac arrest (OHCA) [CoSTR 2017, EvUp 2022, weak recommendation, low-certainty evidence].
A systematic review performed as part of the ILCOR 2025 process1 found that there was insufficient evidence to support a treatment recommendation regarding the optimal order of commencing CPR in children (i.e. providing rescue ventilations or compressions first).
ANZCOR suggest that external cardiac compression should be started while rescuers wait for a bag-mask ventilation (BMV) device to arrive. If a BMV device is immediately available, 2 initial ventilations should be provided before commencement of external cardiac compression [ANZCOR Good Practice Statement].
Starting CPR
The circulation should be assessed by looking for movement, coughing or normal breathing.
Pulse check accuracy was the subject of an ILCOR 2025 PLS Task Force systematic review.1 The review confirmed concerns about low accuracy (sensitivity and specificity) of pulse palpation and potential delays in commencing CPR.
Palpation of a pulse (or its absence) is not reliable as the sole determinant of cardiac arrest and need for chest compressions [CoSTR 2025, weak recommendation, very low-certainty on evidence].
ANZCOR suggest that in infants and children who are unresponsive and breathing is absent (or agonal), healthcare providers should begin CPR [ILCOR Good Practice Statement].
Pulse checks (up to 10 seconds) may still be used as part of the assessment for return of spontaneous circulation (ROSC) and assessment of potentially perfusing rhythms e.g. to define pulseless electrical activity (PEA).
To give chest compressions, the child should be placed on a firm surface and compression directed to the lower half of the sternum.
Compression depth & release
A scoping review was conducted as part of the 2020 ILCOR PLS Task Force process15, 16 to identify new evidence since the 2015 guidelines20, 21 regarding paediatric chest compression depth. No new published evidence was identified with this scoping review, but the PLS Task Force did identify ongoing large prospective observational international multicentre studies on CPR certainty using dual-sensor CPR feedback devices by the pediRES-Q collaborative (https://www.pedires-q.org). Results from these studies are not yet available. As a result, treatment recommendations are unchanged from 201520, 21.
ANZCOR suggest that rescuers compress the chest by at least one third the anteroposterior dimension, or approximately 4cm in an infant and 5cm in a child [CoSTR 2015, weak recommendation, very low-certainty evidence], and up to 5 to 6cm in an adolescent.
Method of compression
An evidence update was performed by the ILCOR 2020 PLS Task Force15, 16, 27to identify available evidence about different techniques for chest compressions of infants and children since the previous review was published in 2010. The evidence update identified several studies published after 2010. A systematic review on this topic is currently underway. Until a new systematic review is completed and analysed by the PLS Task Force, the 2010 treatment recommendation23, 24, 28 remains in effect.
Infants:
ANZCOR suggest that chest compression for an infant be performed with the two-thumb encircling technique (Figure 6) as it results in consistently greater chest compression depth and less fatigue[ANZCOR Good Practice Statement].
With this technique, the rescuer’s hands encircle the chest, and the thumbs compress the sternum. Care should be taken to avoid restricting chest expansion during inspiration. There is insufficient evidence to make a recommendation for or against the need for a circumferential squeeze of the chest when performing the two-thumb encircling technique for infants15, 16, 27. In the absence of evidence supporting the best way to position the thumbs, the two-thumb encircling technique can be performed with thumbs side-by-side or thumbs overlapping (thumb on thumb). Whatever technique is employed, pressure over the ribs and abdominal viscera should be avoided.

Figure 6: Two-thumb technique in an infant
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
ANZCOR suggest that chest compression for an infant using the heel of one hand (Figure 7) may be considered if the rescuer is unable to achieve optimal compression depth using the two-thumb encircling technique [ANZCOR Good Practice Statement].

Figure 7: One-hand compression technique in infant
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
Children:
ANZCOR suggest that chest compression be performed with the ‘heel’ of one hand (Figure 8) or the two-handed technique (Figure 9) regardless of age to achieve optimal compression depth [ANZCOR Good Practice Statement].
Approximately 50% of a compression cycle should be devoted to compression of the chest and 50% to relaxation to enable full recoil of the chest wall. Incomplete relaxation at the end of compression (‘leaning’ on the chest) should be avoided. Pauses in chest compressions should be minimised.

Figure 8: One handed technique in a child
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]


Figure 9: Two-handed techniques in a child
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
Ratios and rates of compressions and ventilations
If ventilations are provided by any type of mouth or mask technique, breaths should be delivered during a planned pause in chest compressions to allow adequate expansion of the lungs. However, to minimise the pause for lung inflation, chest compression should be recommenced during the expiratory phase of the second inflation.
BLS performed by health professionals unfamiliar with PBLS should follow the sequence of 30 compressions, then 2 ventilations (Refer to ANZCOR Guideline 8). The rate of chest compression is 100 to 120 per minute.
ANZCOR suggest that rescuers trained in PBLS should follow the sequence of 15 compressions, then 2 ventilations for each duty cycle [ANZCOR Good Practice Statement].
Compressions may be commenced first if equipment for bag-mask ventilation is not immediately available.
Defibrillator (including AED)
CPR should continue uninterrupted until help arrives with advanced life support equipment (including a defibrillator). Appropriately sized defibrillator pads should be attached to the child as soon as available.
A systematic review was performed by the ILCOR 2025 PLS Task Force 1 to explore defibrillator pad size and placement in infants and children. No paediatric studies were identified that addressed the questions of defibrillator pad size, orientation or placement. Due to the lack of direct evidence in infants and children, the PLS Task Force used the very low certainty evidence from adult studies to inform recommendations.
ANZCOR suggest that [all ILCOR Good Practice Statements]:
· CPR providers using an AED follow the AED specific guidance and instructions for pads placement in infants and children.
· CPR providers using manual defibrillation in infants and children, place pads in an anterior-posterior position.
The ideal pad size is not known, but the largest size available that still enables good separation between the pads should be chosen to enable good contact with the chest wall.
Ensure that all rescuers are clear of the patient while the defibrillator is delivering shocks or when the defibrillator is being disarmed.
Although a variable dose manual defibrillator is preferred, a automated external defibrillator (AED) may be used for infants and children,1 provided it is able to differentiate shockable from non-shockable rapid paediatric rhythms.
A systematic review was conducted by the ILCOR PLS Task Force in 20229-11, 29 (with a supporting Evidence Update in 2025)1 to explore the use of AEDs for infants and children with OHCA. The review suggested that lay rescuers use an AED for all children >1 year of age who have non-traumatic OHCA (weak recommendation, very low–certainty evidence) but were unable to make a recommendation for or against the use of an AED by lay rescuers for children <1 year of age with non-traumatic OHCA.
ANZCOR suggest that: [all ANZCOR Good Practice Statements]:
· For children older than 8 years, a standard AED with adult pads and dose may be used.
· In children 1 to 8 years, an AED with paediatric pads and paediatric dose attenuation is preferred. If that is not available, a standard AED with adult pads and dose may be used.
· In infants, the recommended method of shock delivery by device is listed in order of preference below. If there is any delay in the availability of the preferred device, the device that is available should be used. The AED algorithm should have demonstrated high specificity and sensitivity for detecting shockable rhythms in infants. The order of preference is as follows:
1. Manual defibrillator
2. AED with dose attenuator
3. AED without dose attenuator
When to stop CPR
ANZCOR suggest that PBLS measures should continue until [all ANZCOR Good Practice Statements]:
· Responsiveness and/or normal breathing return.
· The rescuer becomes exhausted.
· The patient is pronounced deceased by the attending advanced life support team.
Recovery position
An unconscious infant/child who is not in cardiac arrest, whose airway is clear, and who is breathing normally, may be turned onto their side into the recovery position.
The recovery position aims to prevent airway obstruction and reduce the likelihood of fluids (saliva, secretions, blood, or vomit) from entering the upper airway.
- Place the child in as near true lateral position as possible, with the mouth facing downwards, enabling free drainage of fluid.
- Stabilise the position if possible. In an infant, this may require a small pillow or a rolled-up blanket to be placed along the back to maintain the position and prevent rolling into a supine or prone position.
- Avoid pressure on the infant/child’s chest which may impair breathing.
- Reassess breathing regularly to recognise deterioration rapidly.
- Regularly change sides to avoid pressure points (e.g. every 30 minutes).
ANZCOR suggest that, in the setting of trauma, unconscious children should preferably have their airway kept open using a jaw thrust manoeuvre rather than being placed in a recovery position (to avoid spinal rotation) [ANZCOR Good Practice Statement].
Foreign body airway obstruction in children
Foreign Body Airway Obstruction (FBAO) is a life-threatening emergency. Chest thrusts or back blows are effective for relieving FBAO in conscious adults and children with low risk of harm.30, 31 Life-threatening complications associated with the use of abdominal thrusts (including the Heimlich Manoeuvre) have been reported.
The child with an effective cough should be given reassurance and encouragement to keep coughing to expel the foreign material. If the obstruction is not relieved, the rescuer should call for help.
If the cough is ineffective and the child is conscious, perform up to five sharp, back blows with the hand in the middle of the back between the shoulder blades (Figure 10). Check to see if each back blow has relieved the airway obstruction. The aim is to relieve the obstruction with each blow rather than to give all five blows.
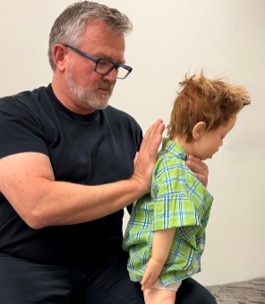
Figure 10: Back blows in child
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
ANZCOR suggest that an infant should be placed in a head downwards position with the head supported (Figure 11) prior to delivering back blows, i.e. across the rescuer’s lap [ANZCOR Good Practice Statement].

Figure 11: Back blows in infant
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
If back blows are unsuccessful the rescuer should perform up to five chest thrusts. To perform chest thrusts, identify the same compression point as for CPR and give up to five chest thrusts. These are similar to chest compressions but sharper and delivered at a slower rate. In an infant, the thumb-encircling technique or even the heel of one hand may provide more effective force for chest thrusts.
ANZCOR suggest that, for chest thrusts, the infant should be placed in a head downwards and on their back across the rescuer’s thigh, while larger children may be treated in the sitting or standing position [ANZCOR Good Practice Statement].
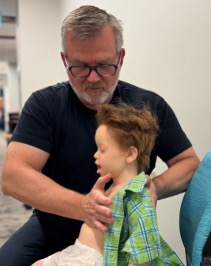

Figure 12: Chest thrusts in child
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]


Figure 13: Chest thrusts in infant
[Image courtesy of Children’s Health Queensland, licensed under CC BY-NC 4.0]
With each chest thrust, check to see whether the airway obstruction has been relieved. The aim is to relieve the obstruction rather than deliver all five chest thrusts. If the obstruction is still not relieved and the person remains responsive, continue alternating five back blows with five chest thrusts.
If the child becomes unresponsive and is not breathing normally, CPR should be commenced.
ANZCOR suggest that the use of back blows and chest thrusts in the management of FBAO in children rather than abdominal thrusts [ANZCOR Good Practice Statement].
ANZCOR suggest against the use of blind finger sweeps. [2020 CoSTR, weak recommendation, very low-certainty evidence]
ANZCOR suggest that rescuers consider the manual extraction of visible items in the mouth. [2020 CoSTR, weak recommendation, very low-certainty evidence]
References
1. Scholefield BR AJ, Ng K-C, Tiwari LK, Raymond TT, Christoff A, and Katzenschlager S E-KR, Bansal A, Topjian A, Kleinman M, Kurosawa H, Myburgh MC, del Castillo J, Rossano J, Djakow J, Guerguerian A-M, Nadkarni VM, Bittencourt Couto T, Schexnayder SM, Nuthall G, Tijssen JA, Ong GY-K, Gray JM, Lopez-Herce J, Ambunda ES, Nolan JP, Berg KM, Morrison LJ, Atkins DL, de Caen AR; on behalf of the Pediatric Life Support Task Force Collaborators. Pediatric life support: 2025 International Liaison Committee on Resuscitation Consensus on Science With Treatment Recommendations. Resuscitation. 2025;215.
2. Djakow J TN, Skellett S, Buysse CMP, Cardona F, de Lucas N, del Castillo J, Kiviranta P, Lauridsen KG, Markel F, Martinez-Mejias A, Roggen I, Biarent D, on behalf of the ERC Paediatric Life Support Writing Group Collaborators. European Resuscitation Council Guidelines 2025 Paediatric Life Support. Resuscitation. 2025;215.
3. Joyner BL DM, Bavare A, de Caen A, DiMaria K, Donofrio-Odmann J, Fosse G, Haskell S, Mahgoub M, Meckler G, Requist J, Schexnayder SM, Olech Smith M, Werho D, Raymond TT. Part 6: pediatric basic life support: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152:S424–S447.
4. Lasa JJ DG, Duff JP, Hayes J, Kamath-Rayne BD, Levy A, Mahgoub M, Morgan RW, McCormick T, Roberts JS, Ross CE, Schexnayder SM, Sweberg T, Valdes SO, Topjian AA. Part 8: pediatric advanced life support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025;152:S479–S537.
5. Greif R, Bray JE, Djarv T, Drennan IR, Liley HG, Ng KC, Cheng A, Douma MJ, Scholefield BR, Smyth M, Weiner G, Abelairas-Gomez C, Acworth J, Anderson N, Atkins DL, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2024;150:e580-e687.
6. Greif R, Bray JE, Djarv T, Drennan IR, Liley HG, Ng KC, Cheng A, Douma MJ, Scholefield BR, Smyth M, Weiner G, Abelairas-Gomez C, Acworth J, Anderson N, Atkins DL, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2024;205:110414.
7. Berg KM, Bray JE, Ng KC, Liley HG, Greif R, Carlson JN, Morley PT, Drennan IR, Smyth M, Scholefield BR, Weiner GM, Cheng A, Djarv T, Abelairas-Gomez C, Acworth J, et al. 2023 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2024;195:109992.
8. Berg KM, Bray JE, Ng KC, Liley HG, Greif R, Carlson JN, Morley PT, Drennan IR, Smyth M, Scholefield BR, Weiner GM, Cheng A, Djarv T, Abelairas-Gomez C, Acworth J, et al. 2023 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2023;148:e187-e280.
9. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, Scholefield BR, Smyth MA, Welsford M, Zideman DA, Acworth J, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Pediatrics. 2023;151.
10. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, Scholefield BR, Smyth MA, Welsford M, Zideman DA, Acworth J, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Resuscitation. 2022;181:208-288.
11. Wyckoff MH, Greif R, Morley PT, Ng KC, Olasveengen TM, Singletary EM, Soar J, Cheng A, Drennan IR, Liley HG, Scholefield BR, Smyth MA, Welsford M, Zideman DA, Acworth J, et al. 2022 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2022;146:e483-e557.
12. Wyckoff MH, Singletary EM, Soar J, Olasveengen TM, Greif R, Liley HG, Zideman D, Bhanji F, Andersen LW, Avis SR, Aziz K, Bendall JC, Berry DC, Borra V, Bottiger BW, et al. 2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group. Circulation. 2022;145:e645-e721.
13. Wyckoff MH, Singletary EM, Soar J, Olasveengen TM, Greif R, Liley HG, Zideman D, Bhanji F, Andersen LW, Avis SR, Aziz K, Bendall JC, Berry DC, Borra V, Bottiger BW, et al. 2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group. Resuscitation. 2021;169:229-311.
14. Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Bittencourt Couto T, Guerguerian AM, Nadkarni VM, Ng KC, Nuthall GA, Ong GYK, Reis AG, Schexnayder SM, Scholefield BR, Tijssen JA, et al. Pediatric Life Support 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Pediatrics. 2021;147.
15. Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Couto TB, Guerguerian AM, Nadkarni VM, Ng KC, Nuthall GA, Ong GYK, Reis AG, Schexnayder SM, Scholefield BR, Tijssen JA, et al. Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation. 2020;156:A120-A155.
16. Maconochie IK, Aickin R, Hazinski MF, Atkins DL, Bingham R, Couto TB, Guerguerian AM, Nadkarni VM, Ng KC, Nuthall GA, Ong GYK, Reis AG, Schexnayder SM, Scholefield BR, Tijssen JA, et al. Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:S140-S184.
17. Soar J, Maconochie I, Wyckoff MH, Olasveengen TM, Singletary EM, Greif R, Aickin R, Bhanji F, Donnino MW, Mancini ME, Wyllie JP, Zideman D, Andersen LW, Atkins DL, Aziz K, et al. 2019 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces. Circulation. 2019;140:e826-e880.
18. Olasveengen TM, de Caen AR, Mancini ME, Maconochie IK, Aickin R, Atkins DL, Berg RA, Bingham RM, Brooks SC, Castren M, Chung SP, Considine J, Couto TB, Escalante R, Gazmuri RJ, et al. 2017 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Summary. Resuscitation. 2017;121:201-214.
19. Olasveengen TM, de Caen AR, Mancini ME, Maconochie IK, Aickin R, Atkins DL, Berg RA, Bingham RM, Brooks SC, Castren M, Chung SP, Considine J, Couto TB, Escalante R, Gazmuri RJ, et al. 2017 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Summary. Circulation. 2017;136:e424-e440.
20. de Caen AR, Maconochie IK, Aickin R, Atkins DL, Biarent D, Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM, Ng KC, Nuthall G, Reis AG, Shimizu N, Tibballs J, et al. Part 6: Pediatric Basic Life Support and Pediatric Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2015;132:S177-203.
21. Maconochie IK, de Caen AR, Aickin R, Atkins DL, Biarent D, Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM, Ng KC, Nuthall G, Reis AG, Shimizu N, Tibballs J, et al. Part 6: Pediatric basic life support and pediatric advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation. 2015;95:e147-68.
22. de Caen AR, Maconochie IK, Aickin R, Atkins DL, Biarent D, Guerguerian AM, Kleinman ME, Kloeck DA, Meaney PA, Nadkarni VM, Ng KC, Nuthall G, Reis AG, Shimizu N, Tibballs J, et al. Part 6: Pediatric Basic Life Support and Pediatric Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations (Reprint). Pediatrics. 2015;136 Suppl 2:S88-119.
23. Kleinman ME, de Caen AR, Chameides L, Atkins DL, Berg RA, Berg MD, Bhanji F, Biarent D, Bingham R, Coovadia AH, Hazinski MF, Hickey RW, Nadkarni VM, Reis AG, Rodriguez-Nunez A, et al. Pediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1261-318.
24. de Caen AR, Kleinman ME, Chameides L, Atkins DL, Berg RA, Berg MD, Bhanji F, Biarent D, Bingham R, Coovadia AH, Hazinski MF, Hickey RW, Nadkarni VM, Reis AG, Rodriguez-Nunez A, et al. Part 10: Paediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation. 2010;81 Suppl 1:e213-59.
25. International Liaison Committee on R. 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Part 6: Paediatric basic and advanced life support. Resuscitation. 2005;67:271-91.
26. Topjian AA, Raymond TT, Atkins D, Chan M, Duff JP, Joyner BL, Jr., Lasa JJ, Lavonas EJ, Levy A, Mahgoub M, Meckler GD, Roberts KE, Sutton RM and Schexnayder SM. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020;142:S469-s523.
27. Maconochie IK AR, Hazinski MF, et al. . Pediatric Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:S140-S184.
28. Kleinman ME, de Caen AR, Chameides L, Atkins DL, Berg RA, Berg MD, Bhanji F, Biarent D, Bingham R, Coovadia AH, Hazinski MF, Hickey RW, Nadkarni VM, Reis AG, Rodriguez-Nunez A, et al. Part 10: Pediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122:S466-515.
29. Atkins DL, Acworth J, Chung SP, Reis A, Van de Voorde P, International Liaison Committee on Resuscitation P and Basic Life Support Task F. Lay rescuer use of automated external defibrillators in infants, children and adolescents: A systematic review. Resusc Plus. 2022;11:100283.
30. Couper K, Abu Hassan A, Ohri V, Patterson E, Tang HT, Bingham R, Olasveengen T, Perkins GD, International Liaison Committee on Resuscitation B and Paediatric Life Support Task Force C. Removal of foreign body airway obstruction: A systematic review of interventions. Resuscitation. 2020;156:174-181.
31. Olasveengen TM, Mancini ME, Perkins GD, Avis S, Brooks S, Castren M, Chung SP, Considine J, Couper K, Escalante R, Hatanaka T, Hung KKC, Kudenchuk P, Lim SH, Nishiyama C, et al. Adult Basic Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2020;142:S41-S91.
Referencing this guideline
When citing the ANZCOR Guidelines we recommend:
ANZCOR, 2026, Guideline 12.1 – Paediatric Basic Life Support (PBLS) for health professionals, accessed 5 August 2026, https://www.anzcor.org/home/paediatric-advanced-life-support/guideline-12-1-paediatric-basic-life-support-pbls-for-health-professionals
