Guideline 9.2.1 – Recognition and First Aid Management of Suspected Heart Attack
Summary
Who does this guideline apply to?
This guideline applies to adults.
Who is the audience for this guideline?
This guideline is for use by bystanders, first aiders and first aid training providers.
Recommendations
The Australian and New Zealand Committee on Resuscitation (ANZCOR) makes the following recommendations:
- First aiders should send for an ambulance if symptoms are severe, get worse quickly or last longer than 10 minutes. [Good Practice Statement]
- First aiders should stay with the person until the ambulance or on-site resuscitation team takes over care. [Good Practice Statement]
- We suggest that first aiders give aspirin (300 mg orally to adults with non-traumatic chest pain unless the person has known anaphylaxis to aspirin. 1 [CoSTR 2020: weak recommendation, very low certainty evidence]
Abbreviations
|
Abbreviation |
Meaning/Phrase |
|
ANZCOR |
Australian and New Zealand Committee on Resuscitation |
|
CoSTR |
Consensus on Science with Treatment Recommendations (from International Liaison Committee on Resuscitation - ILCOR) |
|
AED |
Automated External Defibrillator |
Introduction
A person experiences a heart attack when there is a sudden partial or complete blockage of one of the coronary arteries that supply the heart muscle. As a result of the interruption to the blood supply, there is an immediate risk of life-threatening changes to the heart rhythm. If not corrected quickly there is also a risk of serious, permanent heart muscle damage. To reduce the chance of sudden death from heart attack, urgent medical care is required – “every minute counts”.
Heart attack is different from, but may lead to, cardiac arrest. Cardiac arrest is cessation of heart action.
Survival after heart attack can be improved by current treatments1 and clot-dissolving medications that clear the blocked artery, restore blood supply to the heart muscle and limit damage to the heart. These therapies are most effective if administered as soon as possible following the onset of symptoms with these benefits declining with delays in treatment.
Recognition
For some people, sudden cardiac arrest may occur as the first sign of heart attack – however most experience some warning signs. It is important to note:
- a heart attack can occur in a person without chest pain or discomfort. The most common symptom of heart attack in a person without chest pain is shortness of breath
- a person who experiences a heart attack may pass off their symptoms as ‘just indigestion’
Warning signs/Red Flags
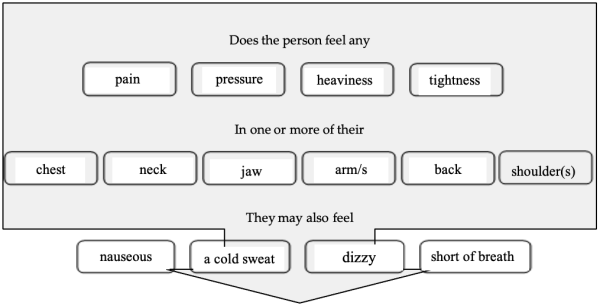
If the warning signs are severe, get worse quickly, or last longer than 10 minutes, act immediately. The person may experience one or more of these symptoms:
- pain or discomfort in the chest, neck, jaw or arms
- pale skin
- shortness of breath
- nausea or vomiting
- sweating
- feeling dizzy or light-headed.
Discomfort or pain in the centre of the chest may start suddenly or come on slowly over minutes. It may be described as tightness, heaviness, fullness or squeezing. The pain may be severe, moderate or mild. The pain may be limited to, or spread to, the neck, throat, jaw, either or both shoulders, the back, either or both arms and into the wrists and hands.
Atypical chest pain is defined as pain that does not have a heaviness or squeezing sensation (typical angina symptoms), precipitating factors (e.g., exertion), or usual location.
Some people are more likely to describe atypical2 or minimal symptoms3 and include:
- the elderly
- women
- people with diabetes and/or chronic inflammatory conditions (eg Rheumatoid arthritis)
- Aboriginal and Torres Straight Islanders, Māori and Pasifika people
These people should seek urgent assessment by a health care professional if they have any warning signs of heart attack, no matter how mild.
Management
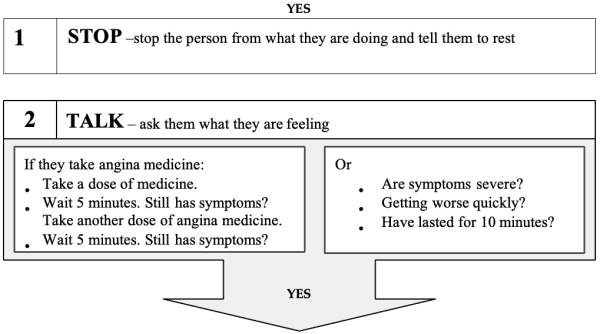
- Encourage the person to stop what they are doing and to rest in a comfortable position.
- If the person has been prescribed medication such as a tablet or oral spray to treat episodes of chest pain or discomfort associated with angina, assist them to take this as they have been directed.
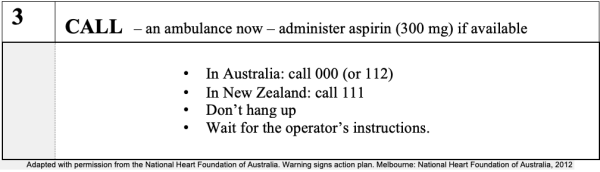
- Send for an ambulance if symptoms are severe, get worse quickly or last longer than 10 minutes.
- Follow the instructions of the ambulance call taker/operator who will advise you what to do.
- Stay with the person until the ambulance or on-site resuscitation team arrives.
- ANZCOR suggests to give aspirin (300 mg orally to adults with non-traumatic chest pain unless the person has known anaphylaxis to aspirin [CoSTR 2020: weak recommendation, very low certainty evidence]
- ANZCOR suggests against the routine administration of oxygen in persons with suspected heart attack. [COSTR 2015, weak recommendation, very-low certainty evidence]Administer oxygen only if there are obvious signs of shock or evidence of low oxygen saturation according to [Refer to ANZCOR Guideline 9.2.10]5,6
- If practical and resources allow, locate the closest AED and bring it to the person.
If the person is unresponsive and not breathing normally, commence resuscitation following the Basic Life Support Flowchart [Refer to ANZCOR Guideline 8].
Warning Signs of Heart Attack Action Plan
References
- Djarv T, Swain J M, Chang W, et al. (February 03, 2020) Early or First Aid Administration Versus Late or In-hospital Administration of Aspirin for Non-traumatic Adult Chest Pain: A Systematic Review. Cureus 12(2): e6862. doi:10.7759/cureus.6862
- 2011 Addendum to the National Heart Foundation/Cardiac Society of Australia and New Zealand Guidelines for the Management of Acute Coronary Syndromes (ACS) 2006. Heart, Lung and Circulation Volume 20, Issue 8, Aug 2011, Pages 487–502
- Patel H, Rosengren A, Ekman I, et al. (2004) Symptoms in acute coronary syndromes: Does sex make a difference? American Heart Journal. 148(1):27-33.
- Canto J, Rogers W, Goldberg R, et al. (2012) Association of Age and Sex With Myocardial Infarction Symptom Presentation and In-Hospital Mortality. Journal of the American Medical Association. 307(8):813-822
- Nikolaou NI, Welsford M, Beygui F, et al. Part 5: Acute coronary syndromes 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation2015; 95: e121-e46.
- Chew D, Scott I, Cullen L, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016. Med J Aust2016; 205(3): 128
Further Reading
- National Heart Foundation (Australia). Heart Attack Facts. http://www.heartattackfacts.org.au
- National Heart Foundation (Australia) Warning signs of heart attack action plan. http://www.heartattackfacts.org.au/action_plans/HeartAttackActionPlan-english.pdf
- ANZCOR Guideline 7 External Automated Defibrillation in Basic Life Support
- ANZCOR Guideline 8 Cardiopulmonary Resuscitation
- ANZCOR Guideline 14 ACS: Overview & summary
- ANZCOR Guideline 14.1 ACS: Presentation with ACS
- ANZCOR Guideline 14.2 ACS: Initial Medical Therapy
About this Guideline:
|
Search date/s |
October 2020 |
|
Question/PICO: |
Population: Adults who experience non-traumatic chest pain Intervention: early or first aid administration of aspirin Comparators: late or in-hospital administration of aspirin Outcomes: Survival, complications and incidence of cardiac arrest were ranked as critical outcomes. Cardiac functional outcome, infarct size and chest pain resolution were ranked as important outcomes. Study Designs: Randomized controlled trials (RCTs) and non-randomized studies (non-randomized controlled trials, interrupted time series, controlled before-and-after studies, cohort studies), case series of 5 or more subjects were eligible for inclusion. Unpublished studies (e.g., conference abstracts, trial protocols) were excluded. Timeframe: All years and all languages were included; unpublished studies (e.g., conference abstracts, trial protocols) were excluded. Literature search updated to October 22, 2019. |
|
Method: |
Systematic Review (ILCOR First Aid Task Force, CoSTR) search in 2019 |
|
Primary reviewers: |
Natalie Hood, Finlay Macneil |
|
Other consultation: |
Dion Stub |
|
Worksheet: |
|
|
Approved: |
April 2021 |
|
Guideline superseded: |
ANZCOR Guideline 9.2.1 - August 2016 |
Referencing this guideline
When citing the ANZCOR Guidelines we recommend:
ANZCOR, 2026, Guideline 9.2.1 – Recognition and First Aid Management of Suspected Heart Attack, accessed 28 July 2026, https://www.anzcor.org/home/first-aid/guideline-9-2-1-recognition-and-first-aid-management-of-suspected-heart-attack
